What Is Asynchronous Mental Health Care?
Written by Klarity Editorial Team
Published: Jul 6, 2026

Asynchronous mental health care is a therapy model where patients and providers exchange written messages at different times, with no requirement for both parties to be online simultaneously. This approach, sometimes called message-based psychotherapy in clinical literature, sits at the center of a growing shift in how people access mental health support. Research published in JAMA Network Open confirms that message-based psychotherapy produces clinical remission rates comparable to video-based therapy for mild to moderate depression and anxiety. For anyone with an unpredictable schedule, social anxiety, or limited access to in-person care, this model offers a real and evidence-backed path to treatment.
What is asynchronous mental health care and how does it work?
Asynchronous mental health care works through structured, message-based exchanges on secure digital platforms. A patient writes a message describing their thoughts, feelings, or progress. The therapist reads it, formulates a clinical response, and replies within a defined window, typically 24 to 48 hours. Neither party needs to be available at the same moment.
The communication flow mirrors traditional therapy in purpose but differs in format. A therapist might ask a patient to journal about a triggering event, then respond with a cognitive behavioral technique to reframe the thought. The patient applies the technique, writes back with observations, and the cycle continues. This back-and-forth builds a permanent therapeutic record that both parties can review to track progress and deepen insight.

Platforms used for this type of care must meet HIPAA-compliance standards. Standard email is not appropriate. Dedicated clinical messaging systems, secure patient portals, and telehealth platforms with encrypted messaging are the correct tools. The American Telemedicine Association recognizes asynchronous virtual care as a distinct and legitimate delivery model within telehealth.
Structure is non-negotiable in this format. According to clinical practice guidance, defined communication boundaries protect both patient and provider from boundary erosion and clinician burnout. Therapists set explicit rules about message length, response windows, and what constitutes a crisis requiring immediate escalation to a phone call or emergency services.
- Messages are exchanged on a defined schedule, not as open-ended texting
- Response windows are agreed upon in advance, typically 24 to 48 hours
- Crisis protocols are established before therapy begins
- Platform security must meet HIPAA standards
- Message length and content expectations are set at intake
Pro Tip: Asynchronous therapy is not a 24/7 open chat line. Therapists respond within agreed windows, and patients should treat each message as a structured clinical communication, not a casual text.
What are the benefits of asynchronous mental health care?
Flexibility is the most immediate benefit, but the clinical case goes deeper. Asynchronous therapy reduces treatment dropout rates by up to 40% compared to traditional in-person therapy. That figure reflects a real problem: patients miss appointments, lose momentum, and disengage. A model that fits around unpredictable schedules removes one of the most common barriers to sustained care.
Written communication also creates a unique therapeutic advantage. When you write about an emotional experience, you process it differently than when you speak about it in real time. The act of composing a message requires reflection, which itself has therapeutic value. The permanent written record that accumulates over weeks of messaging becomes a tool for tracking patterns, reviewing progress, and reinforcing coping strategies.
“Text-based asynchronous communication can reduce anxiety for clients who struggle with live sessions and provides privacy by allowing therapy communications to be less visible to others, contributing to patient comfort and willingness to disclose sensitive information.”
— Clinical insight on asynchronous care, Kicks Therapy
For patients with social anxiety, the absence of real-time social pressure is significant. There is no need to manage facial expressions, voice tone, or the discomfort of silence. Many patients disclose more in writing than they would in a live session. That increased disclosure can accelerate therapeutic progress.
- Flexible scheduling fits around work, caregiving, and irregular routines
- Reduced dropout rates improve long-term treatment outcomes
- Written reflection deepens self-awareness between sessions
- Lower social pressure encourages more honest disclosure
- Immediate access to care reduces wait times compared to appointment-only models
What are the limitations and best use cases for this therapy format?
Asynchronous therapy is not the right fit for every patient or every condition. Severe mental health conditions, active suicidal ideation, psychosis, and complex trauma all require real-time emotional attunement that written messages cannot replicate. A therapist cannot hear a patient’s voice crack or observe body language through text. Those cues carry clinical information that matters.
Standalone asynchronous therapy also shows higher attrition rates than synchronous formats. When patients receive limited real-time feedback, motivation can drop. The absence of a live human presence removes an accountability structure that many patients rely on to stay engaged. This is why hybrid models, combining asynchronous messaging with periodic live sessions, consistently produce better outcomes than either format alone.
Patients who thrive in asynchronous therapy tend to share specific traits. Strong written articulacy and self-reflection are the clearest predictors of success. If you struggle to express yourself in writing or find it hard to identify your own emotional states without prompting, a live session may serve you better as a starting point.
- Asynchronous therapy works best for mild to moderate anxiety, depression, and stress
- Not appropriate as a sole modality for severe conditions or active crises
- Patients with strong writing skills and self-awareness engage most effectively
- Hybrid approaches combining messaging and live sessions optimize outcomes
- Complex trauma and grief often require real-time emotional processing
Pro Tip: Before starting asynchronous therapy, establish a written communication agreement with your therapist. Agree on response times, message length, and the exact protocol for crisis situations. This agreement protects both of you.
How to get started with asynchronous mental health care
Starting asynchronous therapy requires more intentional setup than booking a standard appointment. The structure you establish at the beginning determines how effective the experience will be. Follow these steps to set yourself up for success.
- Choose a HIPAA-compliant platform. Standard email and consumer messaging apps do not meet clinical privacy standards. Use a dedicated telehealth platform or secure patient portal. Helloklarity connects patients with licensed online providers who operate within compliant systems.
- Set communication expectations upfront. Agree with your therapist on how often you will message, how long responses will take, and what topics are appropriate for text versus a live call. This agreement prevents confusion and keeps the therapy structured.
- Write with intention. Treat each message as a clinical document, not a casual note. Describe the situation, your emotional response, and any patterns you notice. Specific detail gives your therapist more to work with.
- Review past messages regularly. The written record is one of asynchronous therapy’s greatest assets. Re-reading previous exchanges helps you track progress, identify recurring patterns, and reinforce what you have learned. This practice deepens the role of technology in mental health by turning a passive record into an active tool.
- Address motivation dips early. If you notice yourself delaying messages or losing interest, tell your therapist directly. Research shows that maintaining engagement requires early communication rhythm agreements. Raising the issue early prevents dropout.
- Know when to escalate. Asynchronous therapy is not crisis care. If your mental state deteriorates rapidly, contact a crisis line or request a live session. Your communication agreement should already specify this protocol.
For a broader picture of what remote therapy involves, the Helloklarity guide on online therapy expectations covers the full scope of virtual mental health support options.
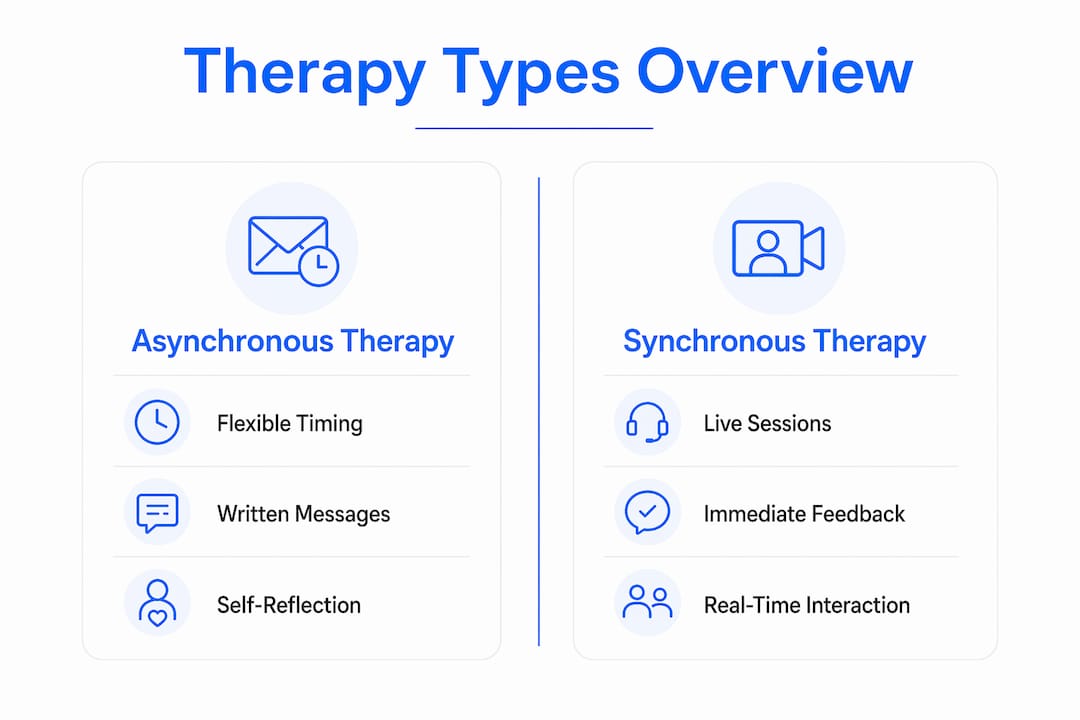
How does asynchronous therapy compare to synchronous therapy?
The core difference is timing. Synchronous therapy requires both patient and therapist to be present at the same time, whether in person or on a video call. Asynchronous therapy removes that requirement entirely. Both formats deliver clinical value, but they serve different needs.
Research from JAMA Network Open shows that message-based therapy produces outcomes comparable to video therapy for mild to moderate depression and anxiety over 5–12 week trials. That finding matters because it validates asynchronous care as a genuine clinical tool, not a lesser substitute. For more complex conditions, synchronous formats retain a clear advantage because they allow real-time emotional attunement and immediate clinical response.
| Feature | Asynchronous therapy | Synchronous therapy |
|---|---|---|
| Scheduling | Flexible, no fixed appointment | Fixed appointment required |
| Communication | Written messages, delayed response | Real-time voice or video |
| Best for | Mild to moderate conditions | Moderate to severe conditions |
| Dropout risk | Higher without hybrid support | Lower with regular sessions |
| Written record | Permanent, reviewable | Limited or none |
| Crisis suitability | Not appropriate | Appropriate with protocols |
The most effective approach for many patients is a hybrid model. Text-based messaging handles documentation, reflection, and between-session support. Live sessions handle deeper processing, emotional attunement, and clinical assessment. Hybrid approaches combining both modalities consistently outperform either format used alone.
Key Takeaways
Asynchronous mental health care is a clinically validated, flexible therapy model that works best for mild to moderate conditions when paired with clear communication boundaries and, where needed, live session support.
| Point | Details |
|---|---|
| Clinical effectiveness | Message-based therapy matches video therapy outcomes for mild to moderate depression and anxiety. |
| Dropout reduction | Flexible scheduling reduces treatment dropout rates by up to 40% compared to in-person care. |
| Structure is required | Clear communication agreements on timing, content, and crisis protocols are non-negotiable. |
| Best-fit patients | Patients with strong writing skills and self-reflection capacity engage most successfully. |
| Hybrid models win | Combining asynchronous messaging with live sessions produces the best overall outcomes. |
The case for intentional asynchronous care
I have spent years watching patients drop out of therapy not because the treatment failed them, but because the format did. A standing weekly appointment at 2:00 PM on a Tuesday sounds manageable until you have a demanding job, a child with an unpredictable schedule, or a condition that makes leaving the house genuinely hard. The appointment becomes a source of stress rather than relief, and eventually it gets canceled and never rebooked.
Asynchronous therapy solves that specific problem well. What I find most compelling is the written record. Patients rarely remember what they said in a session three weeks ago. But a message thread is permanent. Re-reading your own words from a difficult moment, weeks later when you are in a better place, is one of the most underrated tools in mental health care. It shows you that you moved through something. That evidence matters.
The risk I see most often is treating asynchronous therapy as a casual check-in rather than a clinical modality. When patients write vague, brief messages and therapists respond with generic encouragement, nothing therapeutic happens. The format only works when both parties treat it with the same intentionality they would bring to a live session. That means structured messages, clinical responses, and a clear agreement about what this communication is for.
My honest recommendation is a hybrid approach for most patients. Use asynchronous messaging to capture thoughts between sessions, track patterns, and maintain momentum. Use live sessions to process the material that needs a real human presence. Neither format alone is as powerful as both used together. The clinical evidence on hybrid models backs this up, and so does practical experience.
— Guorui
Flexible mental health care is available through Helloklarity
Helloklarity connects patients with over 1,000 licensed providers who specialize in mental health conditions including anxiety, depression, and ADHD. The platform offers same-day access, with most patients seeing a provider within 24 hours. Self-pay options start at $49, and Helloklarity accepts major insurance plans and health savings accounts.
Whether you are exploring asynchronous messaging as part of your care or looking for a live telehealth appointment, Helloklarity’s telehealth services cover a full range of mental health options. You can also browse conditions treated on the platform to find the right fit for your specific needs. Getting started takes minutes, and care is available nationwide.
FAQ
What is asynchronous mental health care in simple terms?
Asynchronous mental health care is therapy conducted through written messages that patients and providers exchange at different times, with no need to be online simultaneously. It is a structured clinical format, not casual texting.
Is asynchronous therapy as effective as video therapy?
For mild to moderate depression and anxiety, message-based therapy produces clinical outcomes comparable to video-based therapy in trials lasting 5–12 weeks. It is less suitable for severe or complex conditions.
Who is asynchronous therapy best suited for?
Patients with mild to moderate conditions, strong writing skills, and the ability to self-reflect tend to benefit most. It is particularly useful for people with unpredictable schedules or social anxiety around live sessions.
Does asynchronous therapy work for depression?
Yes. Clinical research confirms that message-based psychotherapy produces remission rates comparable to synchronous video therapy for mild to moderate depression. A hybrid model combining messaging with live sessions often produces the strongest results.
What platforms are safe for asynchronous mental health care?
Only HIPAA-compliant platforms are appropriate for clinical mental health messaging. Dedicated telehealth platforms and secure patient portals meet this standard. Standard email and consumer messaging apps do not.
Recommended
- Asynchronous Primary Care Messaging Explained
- Same-Day Mental Health Care: What You Need To Know
- Mental Health Awareness Month 2026: Why More Americans Are Turning To Telehealth For Anxiety And Depression | Klarity Health, Inc
- The Role Of Technology In Mental Health Access
Get expert care from top-rated providers
Find the right provider for your needs — select your state to find expert care near you.
Related posts






— Monday to Friday, 7:00 AM to 4:00 PM PST
Join our mailing list for exclusive healthcare updates and tips.

— Monday to Friday, 7:00 AM to 4:00 PM PST