The Role of Lifestyle Medicine in Primary Care
Written by Klarity Editorial Team
Published: Jul 2, 2026

Lifestyle medicine is an evidence-based discipline that uses therapeutic lifestyle interventions as the primary method to prevent, treat, and sometimes reverse chronic disease within primary care settings. The role of lifestyle medicine in primary care has grown from a fringe idea into a clinical standard backed by the American College of Lifestyle Medicine (ACLM), the American Academy of Family Physicians (AAFP), and the CDC. It operates through six foundational pillars: nutrition, physical activity, sleep, substance avoidance, social connectedness, and stress management. Each pillar addresses a root cause of the chronic conditions that now drive the majority of healthcare spending in the United States.
What is the role of lifestyle medicine in primary care?
Lifestyle medicine sits at the intersection of prevention and treatment. It is not a wellness trend. The ACLM formally defines it as an evidence-based specialty that uses therapeutic lifestyle change as a first-line clinical intervention, not a supplement to medication.
Chronic noncommunicable diseases, including type 2 diabetes, hypertension, obesity, and cardiovascular disease, share common behavioral root causes. Addressing those causes directly is the core premise. Primary care is the natural home for this work because it is where most patients first present, and where long-term relationships between patients and clinicians develop.

The primary care physician’s role has expanded significantly as a result. Clinicians are now expected to screen for lifestyle risk factors, counsel patients on behavior change, and coordinate multidisciplinary support. That shift requires both clinical tools and a different way of structuring appointments.
What are the six pillars of lifestyle medicine and their impact in primary care?
Each of the six pillars carries independent clinical evidence and interacts with the others to produce compounding benefits.
- Nutrition: A whole-food, plant-predominant diet reduces inflammation, improves glycemic control, and lowers cardiovascular risk. The AAFP’s 2026 obesity management guidelines identify dietary change as the first-line intervention before pharmacotherapy.
- Physical activity: The evidence-based target is 150 minutes per week of moderate-intensity activity or 75 minutes of vigorous activity. Meeting this threshold reduces all-cause mortality and improves blood pressure, insulin sensitivity, and mental health.
- Restorative sleep: Chronic sleep deprivation drives weight gain, impairs immune function, and worsens mood disorders. Primary care screening for sleep quality is now embedded in several clinical guidelines.
- Substance avoidance: Tobacco cessation, limiting alcohol, and avoiding recreational drugs are not optional lifestyle suggestions. They are clinical interventions with measurable outcomes in cancer, liver disease, and cardiovascular risk reduction.
- Social connectedness: Social isolation carries a mortality risk comparable to smoking 15 cigarettes per day, according to public health research. Primary care teams increasingly use social prescribing to connect patients with community resources.
- Stress management: Chronic psychological stress activates inflammatory pathways linked to hypertension, diabetes, and depression. Techniques like mindfulness-based stress reduction (MBSR) and cognitive behavioral therapy (CBT) have clinical trial support.
Pro Tip: Address all six pillars in every chronic disease review, not just the ones most obviously linked to the diagnosis. A patient with hypertension may benefit as much from sleep screening as from dietary advice.
How is lifestyle medicine integrated into primary care workflows?
Embedding lifestyle medicine into standard care requires more than clinician willingness. It requires structural changes to how appointments are designed, who delivers care, and how outcomes are tracked.
Team-based care models
Multidisciplinary teams are the backbone of effective lifestyle medicine delivery. Clearly defined team roles are what separate sustainable programs from one-time initiatives. A functional team typically includes:
- A primary care physician or nurse practitioner who screens, diagnoses, and sets clinical goals.
- A health coach or behavioral health specialist who supports behavior change between visits.
- A registered dietitian who provides medical nutrition therapy for conditions like diabetes and obesity.
- A social prescriber or care coordinator who connects patients to community exercise programs, food banks, or mental health services.
This model distributes the workload so that no single clinician carries the full burden of lifestyle counseling within a 15-minute appointment.
Digital tools and EHR integration
The ACLM’s Whole Person Health Index (LMWPHI) is a structured assessment tool built into Epic EHR systems. Patients complete it before or during a visit, giving clinicians a real-time snapshot across all six pillars. This kind of embedded screening removes the need for ad hoc questioning and creates a documented baseline for follow-up.
Telehealth has also expanded access to lifestyle medicine. Group programs delivered via video, digital coaching apps, and remote monitoring tools allow patients to receive ongoing support without requiring in-person visits at every touchpoint. For patients managing common chronic conditions like hypertension or prediabetes, this continuity is clinically meaningful.
Pro Tip: Treat lifestyle medicine as a longitudinal care pathway with scheduled follow-ups, not a one-time conversation. Patients who receive structured check-ins show significantly better adherence than those who receive advice once.
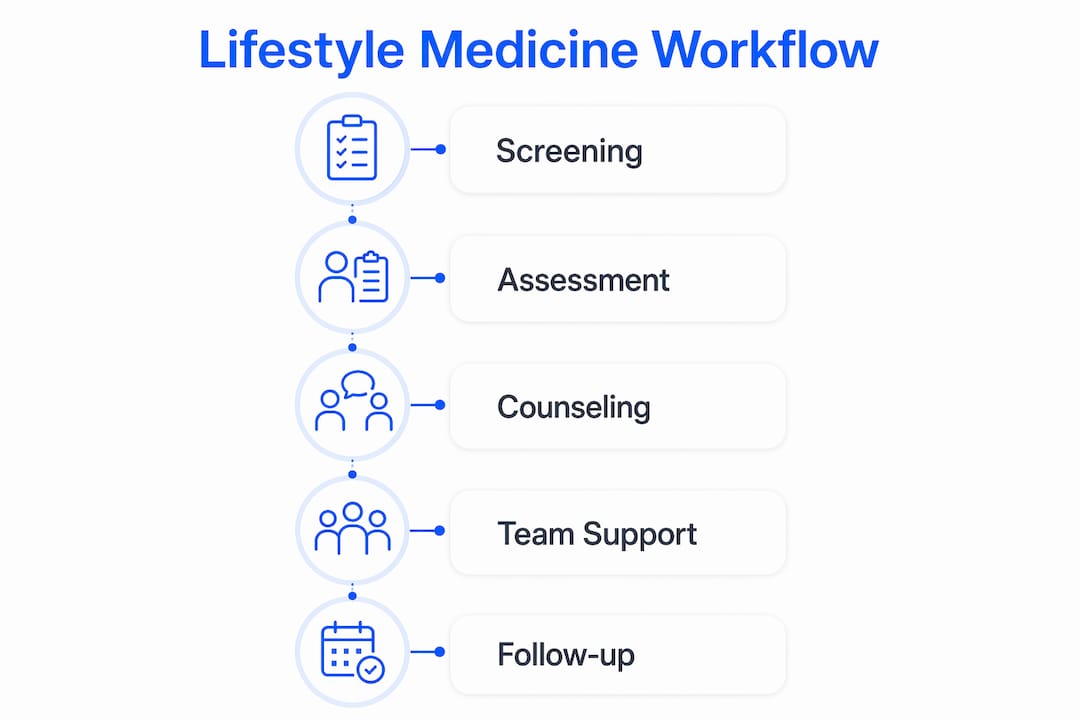
What a structured lifestyle visit looks like
| Component | Description | Time Required |
|---|---|---|
| Lifestyle screening (LMWPHI) | Patient-completed assessment across all six pillars | 5–10 min (pre-visit) |
| Goal-setting conversation | Clinician reviews results and sets one to two behavioral targets | 5–7 min |
| Care team handoff | Warm referral to health coach, dietitian, or social prescriber | 2–3 min |
| Follow-up scheduling | Next check-in booked before patient leaves | 1 min |
What evidence supports lifestyle medicine’s benefits for chronic disease management?
The clinical case for lifestyle medicine in primary care is not theoretical. Controlled trials and large meta-analyses now document outcomes across multiple conditions.
A network meta-analysis of 20 studies involving 5,248 participants found that combined diet, exercise, and peer support interventions improved both weight and blood pressure control more than routine care alone in patients with hypertension and obesity. The finding matters because it confirms that combining pillars produces better results than addressing any single behavior in isolation.
For weight management specifically, structured lifestyle interventions produce 5%–10% weight loss over six months when delivered by multidisciplinary teams with measurable goals. That level of weight loss is clinically significant. It reduces the risk of type 2 diabetes, lowers blood pressure, and improves lipid profiles without pharmacotherapy.
Key evidence-backed outcomes include:
- Type 2 diabetes prevention: Intensive lifestyle programs reduce diabetes incidence by more than 50% in high-risk patients, according to the CDC’s National Diabetes Prevention Program data.
- Hypertension control: Dietary approaches like the DASH diet, combined with physical activity, reduce systolic blood pressure by clinically meaningful margins without medication changes.
- Mental health: Regular physical activity reduces depressive symptoms with effect sizes comparable to antidepressant therapy in mild to moderate depression.
- Cardiovascular risk: Tobacco cessation combined with dietary change and exercise reduces 10-year cardiovascular risk scores substantially in primary prevention populations.
“Lifestyle medicine complements rather than replaces standard care. Behavior-change approaches tailored to patient readiness and context produce the most durable outcomes.” — PMC Comprehensive Review, 2026
What are the barriers and enablers to adopting lifestyle medicine?
The evidence is strong. The adoption is uneven. Understanding why requires looking at system design, not just clinician behavior.
Common barriers
- Time constraints: Standard primary care appointments average 15–20 minutes. Comprehensive lifestyle counseling across six pillars cannot fit into that window without structural support.
- Fee-for-service financing: System-level mismatches like fee-for-service models financially reward procedures and prescriptions over counseling and prevention. This is the most significant structural barrier to adoption.
- Limited clinician training: Most medical school curricula dedicate fewer than 25 hours to nutrition education. Clinicians often lack confidence in delivering lifestyle counseling.
- Poor community integration: Referral pathways to dietitians, exercise programs, and mental health services are inconsistent across health systems and geographies.
Key enablers and policy momentum
The CMS MAHA ELEVATE program is a $100 million cooperative agreement testing whole-person lifestyle medicine interventions in Medicare populations. It funds up to $3.3 million per recipient over three years and uses randomization to measure impact. This signals federal-level recognition that lifestyle medicine needs dedicated funding infrastructure, not just clinical enthusiasm.
Other enablers include value-based payment models that reward outcomes over volume, multidisciplinary team structures that distribute counseling responsibilities, and digital programs that extend care between visits. The primary care visit structure itself is also evolving to accommodate lifestyle screening as a routine component rather than an add-on.
Key Takeaways
Lifestyle medicine is most effective in primary care when it is embedded as a structured, team-based pathway addressing all six pillars with scheduled follow-up and digital support tools.
| Point | Details |
|---|---|
| Six pillars drive outcomes | Nutrition, activity, sleep, substance avoidance, connectedness, and stress management each carry independent clinical evidence. |
| Team-based delivery works | Health coaches, dietitians, and social prescribers distribute the workload that no single clinician can carry alone. |
| Combined interventions outperform single tips | Diet, exercise, and peer support together improve weight and blood pressure more than any single approach. |
| Structural barriers matter most | Fee-for-service financing hinders adoption more than clinician resistance; payment reform is the critical lever. |
| Digital tools extend reach | EHR-integrated screening tools like LMWPHI and telehealth programs improve clinical adoption and patient adherence. |
Why lifestyle medicine needs system change, not just clinical champions
I have watched lifestyle medicine go from a niche interest to a recognized clinical discipline over the past decade. The science was never the problem. The problem has always been the system around the clinician.
The most common mistake I see is treating lifestyle medicine as something a motivated physician does on top of their regular workload. That model burns people out and produces inconsistent results. The practices that succeed are the ones that redesign the workflow first. They build the LMWPHI screening into the intake process. They hire a health coach before they try to train every clinician in behavior change. They schedule follow-ups at the point of care rather than hoping patients will call back.
The fee-for-service problem is real, and the CMS MAHA ELEVATE investment is a genuine signal that policy is catching up. But clinicians should not wait for payment reform to start. Group visit models, telehealth check-ins, and community referral networks can all be built within existing structures if the team is aligned.
The patients who benefit most are not the ones with the most motivation. They are the ones whose care team makes lifestyle support the path of least resistance. That is a design problem, and it is solvable.
— Guorui
Helloklarity’s telehealth services for lifestyle and chronic care
Helloklarity connects patients with licensed primary care providers who take lifestyle medicine seriously. The platform gives you same-day access to over 1,000 providers specializing in weight management, chronic disease, and preventive care, with appointments available within 24 hours.
The Klarity Select Weight Loss Program currently offers $150 off and combines medical oversight with structured lifestyle support aligned with AAFP guidelines. For patients managing hypertension, prediabetes, or obesity, this is a practical entry point into evidence-based care. You can also browse telehealth services by condition or find a licensed provider near you. Self-pay options start at $49, and Helloklarity accepts major insurance and HSA accounts.
FAQ
What is lifestyle medicine in primary care?
Lifestyle medicine is an evidence-based clinical discipline that uses therapeutic changes in nutrition, physical activity, sleep, stress management, substance avoidance, and social connectedness as first-line treatments for chronic disease in primary care settings.
What are the six pillars of lifestyle medicine?
The six pillars are nutrition, physical activity, restorative sleep, avoidance of risky substances, social connectedness, and stress management. Each pillar has independent clinical evidence supporting its role in preventing and managing chronic disease.
How effective are lifestyle interventions for weight loss?
Structured lifestyle interventions delivered by multidisciplinary teams produce 5%–10% weight loss over six months. That level of weight reduction lowers blood pressure, reduces diabetes risk, and improves lipid profiles without requiring medication changes.
What tools help clinicians deliver lifestyle medicine efficiently?
The ACLM’s Lifestyle Medicine Whole Person Health Index (LMWPHI), integrated into Epic EHR systems, allows patients to complete a six-pillar assessment before or during a visit. This gives clinicians a structured baseline without consuming appointment time.
Why is lifestyle medicine not more widely adopted in primary care?
The primary barrier is structural. Fee-for-service payment models reward procedures over counseling, and most primary care appointments are too short for comprehensive lifestyle assessment without team-based support and workflow redesign.
Recommended
- The Role Of Primary Care Physician In Health
- Primary Care Explained: Benefits, Roles, And Services
- What Does A Primary Care Visit Include?
- Common Primary Care Conditions Treated Online: 2026 Guide
Get expert care from top-rated providers
Find the right provider for your needs — select your state to find expert care near you.
Related posts






— Monday to Friday, 7:00 AM to 4:00 PM PST
Join our mailing list for exclusive healthcare updates and tips.

— Monday to Friday, 7:00 AM to 4:00 PM PST