Why Primary Care Shortages Exist: A 2026 Analysis
Written by Klarity Editorial Team
Published: Jul 16, 2026

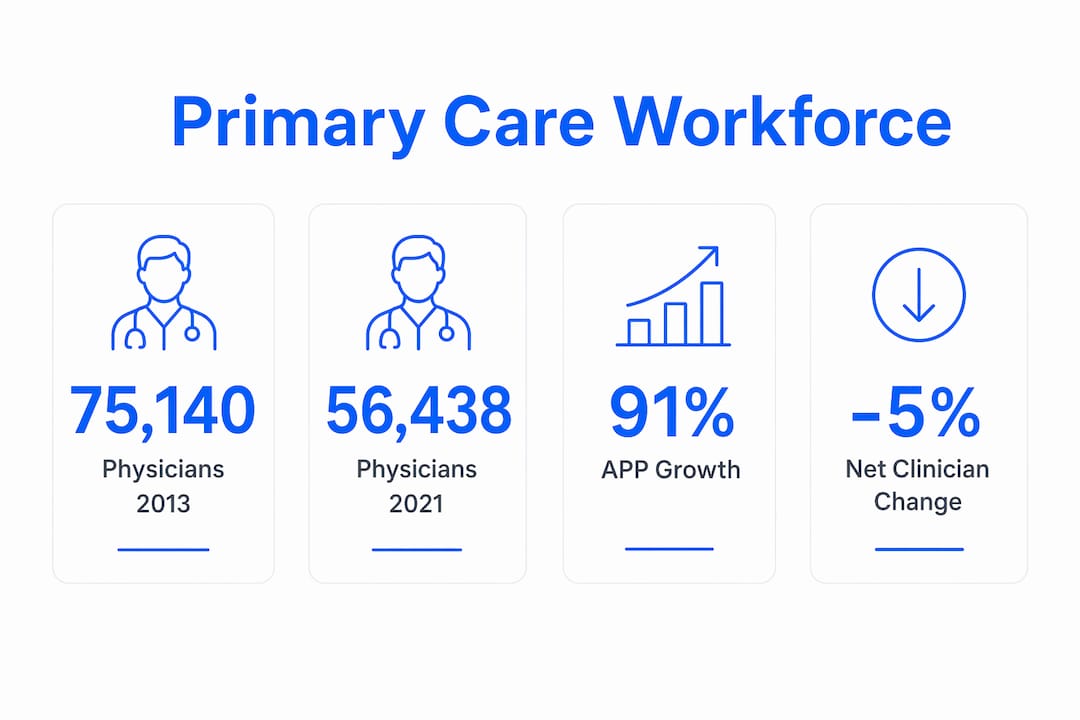
Primary care shortages are defined as a sustained deficit in the number of clinicians available to deliver first-contact, continuous, and coordinated care to the general population. The United States faces a compounding crisis: the number of physicians accepting new patients dropped 23% between 2013 and 2021, falling from 75,140 to 56,438. Understanding why primary care shortages exist requires examining four interlocking forces: declining physician availability, economic disincentives, workforce burnout, and systemic underinvestment. Each factor reinforces the others, making this one of the most structurally stubborn problems in American healthcare.
Why primary care shortages exist: workforce data and trends
The clearest signal of the primary care gap is the collapse in physician availability for new patients. By 2021, fewer than 50% of all primary care physicians were accepting new patients. That means a patient calling a clinic today has roughly even odds of being turned away before the conversation starts.
Advanced Practice Providers (APPs), including nurse practitioners and physician assistants, grew significantly during the same period. APP availability rose 91% between 2013 and 2021, climbing from 12,768 to 24,432 clinicians available for new patient visits. Despite that growth, the net result was still a 5% overall decrease in available primary care clinicians. APPs filled part of the gap, but integration challenges, scope-of-practice restrictions, and supervision requirements limited their ability to fully offset physician losses.
Geographic disparities make the picture worse. The 2026 Primary Care Scorecard from the Milbank Memorial Fund shows workforce density ranging from 86.9 clinicians per 100,000 residents in Nevada to 169.7 per 100,000 in Vermont. A patient in Nevada effectively lives in a different healthcare system than a patient in Vermont. Rural and low-income communities bear the heaviest burden of these gaps.

| Metric | 2013 | 2021/2022 |
|---|---|---|
| Primary care physicians accepting new patients | 75,140 | 56,438 |
| APPs available for new patient visits | 12,768 | 24,432 |
| Adults with no usual source of care | 21% | 30% |
| Clinicians per 100k (Nevada) | Not listed | 86.9 |
| Clinicians per 100k (Vermont) | Not listed | 169.7 |
The table above shows that APP growth, while real, did not reverse the overall decline. The workforce gap is structural, not cyclical.
What economic factors drive primary care gaps?
The economics of primary care actively push physicians toward other specialties. The American Medical Association’s Relative Value Scale Update Committee (RUC) has historically undervalued cognitive primary care services relative to procedural specialties. The result is a salary gap that medical students notice before they choose a residency.
Primary care salaries rank among the lowest of all U.S. medical specialties. A physician who completes the same medical school and residency pathway as a cardiologist or orthopedic surgeon earns substantially less by choosing primary care. That salary gap compounds over a career, especially for graduates carrying significant medical school debt.
The fee-for-service payment model deepens the problem. It rewards volume and procedures over the time-intensive cognitive work that defines primary care: managing chronic disease, coordinating referrals, and counseling patients on prevention. A 15-minute office visit for diabetes management pays far less than a brief procedural intervention in another specialty. Chronic underinvestment in primary care spending, relative to total U.S. health expenditure, reflects this structural bias.
- Low reimbursement rates tied to RUC undervaluation reduce primary care salaries below specialty averages.
- Fee-for-service payment penalizes cognitive, time-intensive work in favor of procedures.
- Medical school debt makes lower-paying primary care careers financially riskier for graduates.
- Administrative overhead consumes unbillable hours, reducing the effective hourly rate further.
Pro Tip: Policymakers evaluating payment reform should examine global primary care spending benchmarks. Countries that invest a higher share of total health spending in primary care consistently achieve better population health outcomes at lower overall cost.
How does burnout reduce the primary care workforce?
Burnout is the mechanism that converts economic pressure into actual workforce loss. Administrative burdens, including complex electronic health records (EHRs) and prior authorization requirements, contribute significantly to burnout and early retirement in primary care. Clinicians who entered medicine to care for patients find themselves spending hours each day on documentation and insurance paperwork instead.
The behavioral response to burnout is predictable. Clinicians limit their clinical scope, shift to part-time schedules, or retire earlier than planned. Each of those decisions removes capacity from an already strained system. A physician who moves from full-time to part-time practice effectively halves their contribution to patient access.
The training pipeline compounds this problem through a negative feedback loop. Medical trainees avoid primary care after observing high burnout and dissatisfaction among current practitioners. The students who shadow a burned-out primary care physician during their clinical rotations draw the obvious conclusion: choose a different specialty. This cycle perpetuates shortages across generations of physicians.
Graduate Medical Education (GME) funding adds another layer of structural failure. CMS and VA funding for GME lacks accountability requirements to produce a sufficient primary care workforce. Hospitals receive federal GME dollars without any mandate to train a specific proportion of primary care physicians. The result is a training system that responds to hospital revenue incentives rather than population health needs.
Pro Tip: Healthcare organizations can reduce burnout-driven attrition by auditing the ratio of clinical hours to administrative hours per clinician. Practices that bring that ratio below 1:3 (administrative to clinical) report meaningfully lower turnover.
For a closer look at how nurse practitioners and physician assistants fit into the solution, the role of primary care providers explains their expanding scope and limitations.
What are the consequences of primary care deficits?
The consequences of primary care scarcity show up directly in population health data. The share of U.S. adults reporting no usual source of care rose from 21% in 2013 to 30% in 2022. That 9-percentage-point increase represents tens of millions of Americans who lack a regular clinician to manage their health.
Patients without a usual source of care delay treatment for chronic conditions. They present to emergency departments with problems that primary care could have caught earlier and at far lower cost. The relationship between primary care access and emergency department visits is well established: fewer primary care visits reliably predict more emergency visits.
Geographic and socioeconomic disparities concentrate these consequences on the most vulnerable populations. Systemic barriers including transportation costs, lack of female clinicians in some communities, and poor patient-staff communication disproportionately affect rural and economically disadvantaged populations. A low-income patient in a rural county faces not just a shortage of clinicians but also the cost of traveling to see one.
- Delayed chronic disease management leads to more hospitalizations and higher long-term costs.
- Increased emergency department use raises system-wide spending without improving outcomes.
- Health disparities widen as rural and low-income communities absorb a disproportionate share of the shortage.
- Preventive care gaps allow conditions like hypertension and diabetes to progress undetected.
Telehealth has begun to address some of these access barriers, particularly for rural patients. The role of telehealth in rural care shows how virtual visits reduce transportation and communication barriers for underserved communities.
Key Takeaways
Primary care shortages exist because economic disincentives, workforce burnout, GME funding gaps, and declining physician availability combine to reduce clinician supply faster than demand grows.
| Point | Details |
|---|---|
| Physician availability collapsed | Primary care physicians accepting new patients dropped 23% between 2013 and 2021. |
| APP growth did not close the gap | A 91% rise in APP availability still produced a net 5% decrease in total primary care clinicians. |
| Economic structure discourages entry | RUC undervaluation of cognitive services keeps primary care salaries among the lowest of all specialties. |
| Burnout accelerates workforce loss | Administrative burden drives early retirement and part-time shifts, reducing available clinical capacity. |
| Access gaps are widening | Adults without a usual source of care increased from 21% to 30% between 2013 and 2022. |
The uncomfortable truth about fixing primary care
The policy conversation around primary care shortages tends to focus on supply: train more physicians, expand APP scope, fund more residency slots. Those interventions matter. But the harder problem is that the system is not broken. It is working exactly as its incentives were designed to work.
Fee-for-service payment rewards procedures. The RUC rewards specialties that perform them. Medical education responds to salary signals. Students choose high-paying specialties. The shortage is the predictable output of a payment system that has never genuinely valued primary care.
What I find most underappreciated in the policy debate is the administrative burden problem. Payment reform gets the headlines, but a primary care physician who spends three hours a day on prior authorizations and EHR documentation is effectively a part-time clinician. You cannot solve a workforce shortage by adding clinicians if the system immediately consumes their capacity in paperwork.
Team-based care models offer a realistic near-term path forward. Embedding medical assistants, care coordinators, and APPs into primary care practices can redistribute administrative tasks and extend physician capacity. The evidence on team-based models is consistent: they reduce burnout, improve patient outcomes, and increase the number of patients a practice can serve.
The long-term fix requires GME accountability. Federal dollars that fund residency training should carry requirements tied to workforce needs, not hospital revenue preferences. Until CMS and the VA attach primary care production targets to GME funding, the training pipeline will continue producing the workforce that hospitals want rather than the one communities need.
— Guorui
Primary care access through Helloklarity
The primary care shortage is a structural problem, but patients still need care today.
Helloklarity connects patients with licensed primary care providers through a telehealth platform that offers same-day appointments. With over 1,000 licensed providers and visits available within 24 hours, Helloklarity addresses the access gap directly. Self-pay options start at $49, and the platform accepts major insurance and health savings accounts. Patients can find a provider by state or browse the full range of conditions treated online to get matched with the right clinician without the wait.
FAQ
Why are fewer primary care physicians accepting new patients?
The number of primary care physicians accepting new patients dropped 23% between 2013 and 2021. Low reimbursement rates, administrative burden, and burnout are the primary drivers of that decline.
Can nurse practitioners and physician assistants replace primary care physicians?
APPs grew 91% between 2013 and 2021 but still produced a net 5% decrease in total available primary care clinicians. Scope-of-practice restrictions and integration challenges limit their ability to fully offset physician shortages.
How does the primary care shortage affect emergency department use?
Patients without a usual source of care are more likely to use emergency departments for conditions that primary care could manage. This increases system-wide costs without improving health outcomes.
What role does medical education play in primary care shortages?
Graduate Medical Education funding from CMS and the VA lacks requirements to produce a sufficient primary care workforce. Medical students also avoid primary care after observing high burnout among current practitioners, creating a self-reinforcing shortage cycle.
What is the fastest way for patients to access primary care today?
Telehealth platforms that offer same-day or next-day appointments provide the most immediate access. Helloklarity offers online primary care visits with licensed providers, with appointments available within 24 hours and self-pay options starting at $49.
Recommended
- Why Primary Care Reduces Emergency Visits: 2026 Guide
- Why Primary Care Is Your First Line Of Defense
- Primary Care Explained: Benefits, Roles, And Services
- Types Of Primary Care Telehealth Services In 2026
Get expert care from top-rated providers
Find the right provider for your needs — select your state to find expert care near you.
Related posts






— Monday to Friday, 7:00 AM to 4:00 PM PST
Join our mailing list for exclusive healthcare updates and tips.

— Monday to Friday, 7:00 AM to 4:00 PM PST