How Telemedicine Billing Codes Work: 2026 Guide
Written by Klarity Editorial Team
Published: Jun 9, 2026
Telemedicine billing codes are the specific CPT codes, HCPCS codes, place of service designators, and modifiers that healthcare providers use to submit claims for virtual care services accurately. Understanding how telemedicine billing codes work is not optional for billing specialists in 2026. It is the difference between clean claims and a denial rate that quietly drains revenue. The core framework involves E/M codes 99202 through 99215, place of service codes 10 and 02, and modifiers 95 and 93, each serving a distinct function in documenting what happened, where, and how during a telehealth encounter.
How telemedicine billing codes work: CPT and HCPCS essentials
Telehealth is not a single billing category. Distinct codes apply for synchronous audio-video visits, audio-only encounters, asynchronous store-and-forward services, and remote patient monitoring. Selecting the wrong code for the wrong modality is one of the most common and preventable billing errors in virtual care.
Standard E/M codes for telehealth visits
CPT codes 99202 through 99215 remain the most frequently used telehealth billing codes, with reimbursement tied to relative value unit (RVU) calculations. CMS fees range from approximately $46 for a level-1 new patient visit up to over $230 for a complex established patient encounter. These codes apply to both in-person and telehealth visits, which means the modality distinction comes from the modifier and place of service code, not the E/M code itself.

For behavioral health, CPT code 90832 covers a 30-minute psychotherapy session, while 90834 and 90837 cover 45-minute and 60-minute sessions respectively. Telephone-only E/M visits use codes 99441 through 99443, tiered by time: 5 to 10 minutes, 11 to 20 minutes, and 21 to 30 minutes. These telephone codes carry lower reimbursement than audio-video equivalents, which makes documenting the technology platform used at the time of service financially significant.
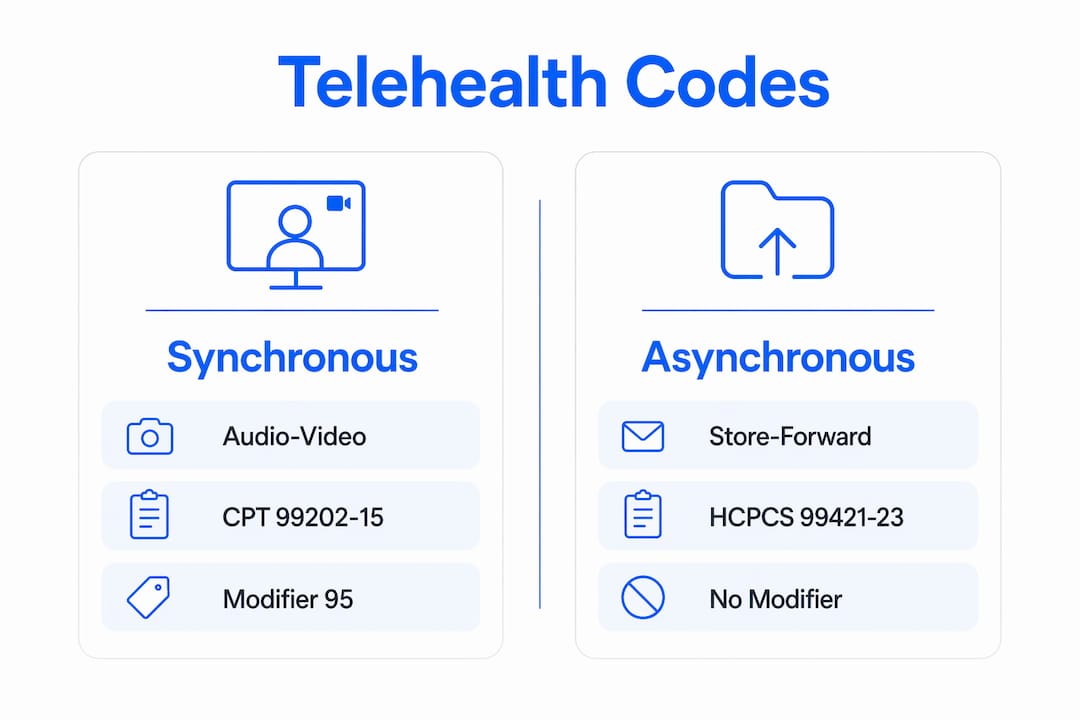
Comparing synchronous vs. asynchronous codes
The table below shows how modality drives code selection:
| Modality | Typical CPT/HCPCS Code | Modifier Required |
|---|---|---|
| Synchronous audio-video | 99202–99215 | 95 |
| Audio-only telephone | 99441–99443 | 93 |
| Asynchronous store-and-forward | G2010, G2012 | None or payer-specific |
| Remote patient monitoring setup | 99453, 99454 | None |
| Remote monitoring management | 99457, 99458 | None |
New telehealth-specific CPT codes in the 98000 series are expanding, but commercial payer adoption is inconsistent. Legacy E/M codes with modifiers remain the safer default until you verify each payer’s accepted code set.
Pro Tip: Build a code-selection decision tree in your practice management system that prompts the scheduler to capture visit modality at booking. This single workflow change prevents the most common mismatch between the service delivered and the code submitted.
How do place of service codes affect telehealth reimbursement?
POS codes 10 and 02 are mandatory for all telehealth claims and carry direct reimbursement consequences. POS 10 designates the patient’s home as the service location. POS 02 designates a non-home originating site such as a clinic, hospital, or federally qualified health center. CMS introduced POS 10 in 2022 specifically to represent home-based telehealth reliably, replacing the previous workaround of using POS 02 for all telehealth encounters.
Why the wrong POS code costs real money
Using POS 02 for patients receiving telehealth at home triggers facility-rate reimbursement rather than the higher non-facility rate. Practices often default to POS 02 because scheduling systems are not configured to capture patient location at the time of booking. The result is systematic underpayment and audit exposure. A single provider seeing 20 telehealth patients per day at the wrong POS rate can lose thousands of dollars monthly without a single claim being formally denied.
Accurate POS coding using POS 10 for home visits versus POS 02 for clinic originating sites directly affects both reimbursement levels and audit risk. CMS auditors specifically flag POS mismatches as indicators of broader documentation failures, which means one incorrect POS code can trigger a broader review of your telehealth claims.
Pro Tip: Add a mandatory patient-location field to your intake workflow and map it directly to the POS code in your billing system. Automate the POS assignment rather than relying on manual entry by billing staff.
What modifiers and documentation are required for claim acceptance?
Modifier 95 is the primary telehealth identifier for synchronous audio-video visits under Medicare Advantage and most commercial payers. Modifier 93 applies to audio-only visits. Some Medicaid programs and legacy payer contracts still require the older GT modifier, which means you cannot apply a single modifier policy across all payers without verification.
Documentation requirements for telehealth claims go beyond what most practices currently capture. CMS and commercial payers require the following elements to be present in the medical record before claim submission:
- Patient location at the time of service, including city and state
- Technology platform used (for example, Zoom for Healthcare, Doxy.me, or a certified EHR telehealth module)
- Provider location at the time of service
- Statement of medical necessity for the telehealth modality
- Documented informed patient consent, including the patient’s right to request in-person care
Missing or incomplete documentation of these elements is the leading cause of claim denial and audit recoupments in 2026. Verbal acknowledgment of consent is not sufficient. CMS and commercial payer audits consistently fail providers who obtained verbal consent but did not document it in writing before or at the time of service, not retroactively.
Documenting medical decision making for E/M code support
For E/M codes, the medical record must support the complexity level billed. Time-based billing requires documentation of total time spent on the date of service, including pre-visit chart review and post-visit care coordination. Medical decision making (MDM) documentation must reflect the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of complications. Clinical documentation must also justify why telehealth was the appropriate modality given the patient’s condition. Payers may deny claims if in-person assessment was medically necessary and telehealth was used instead.
Pro Tip: Create a telehealth-specific documentation template in your EHR that includes mandatory fields for patient location, platform, consent status, and modality justification. A template that cannot be completed without these fields eliminates the most common audit failure points.
How to navigate payer-specific rules and prevent billing denials
Telehealth claim denials between 15 and 20% are frequently caused by improper coding, missing modifiers, or incorrect place of service usage. That denial rate is not random. It reflects a structural problem: billing teams applying Medicare rules to commercial claims, or using last year’s modifier requirements for a payer that updated its policy in January.
Commercial payers display a wide variety of telehealth billing policies requiring customized payer rules frameworks for code, modifier, and documentation requirements. Relying solely on Medicare coding rules causes frequent denials and lost revenue for commercial claims. The following steps reduce denial rates systematically:
- Build a payer-specific crosswalk. For each payer in your contract portfolio, document the accepted telehealth CPT codes, required modifiers, POS requirements, and consent documentation standards. Update this crosswalk at least quarterly.
- Verify coverage before the visit. Confirm that the patient’s plan covers the specific telehealth service being provided, including the modality. Payment parity laws require equal reimbursement for telehealth and in-person visits in many states, but enforcement is inconsistent and payer contracts vary.
- Run pre-submission claim scrubs. Use your clearinghouse or billing software to flag missing modifiers, POS mismatches, and unsupported code combinations before claims leave your system.
- Audit denied claims by denial reason code. Group denials by CO-4 (incorrect procedure code), CO-16 (missing information), and CO-97 (service included in another service) to identify systemic errors rather than treating each denial as a one-off event.
- Train clinical and administrative staff together. Billing errors in telehealth most often originate at the point of scheduling or documentation, not in the billing department. Front-desk staff who understand why patient location matters will capture it consistently.
Pro Tip: Review your Blue Cross Blue Shield telehealth coverage policies separately from your Medicare rules. BCBS plans vary significantly by state and product line, and their modifier requirements for telehealth often differ from CMS guidance.
Key takeaways
Accurate telemedicine billing requires the correct CPT code, the right POS designation, the appropriate modifier, and complete documentation, and every one of these elements must align for a claim to pay on first submission.
| Point | Details |
|---|---|
| CPT code selection by modality | Use 99202–99215 for audio-video E/M, 99441–99443 for telephone-only, and G-codes for store-and-forward services. |
| POS 10 vs. POS 02 | POS 10 is required for home-based telehealth; using POS 02 by default triggers underpayment and audit risk. |
| Modifier accuracy | Modifier 95 covers synchronous audio-video; modifier 93 covers audio-only; verify GT requirements for Medicaid payers. |
| Documentation before billing | Patient location, platform, consent, and modality justification must be in the record before claim submission, not after. |
| Payer-specific crosswalks | Medicare rules do not apply to commercial claims; maintain a separate crosswalk for each payer contract. |
What I’ve learned from watching telehealth billing go wrong
The single most expensive mistake I see practices make is treating telehealth billing as a simple extension of in-person billing. It is not. The code may be the same 99214, but the modifier, the POS code, the consent documentation, and the modality justification are all additional layers that in-person billing never required. Practices that bolt telehealth onto their existing workflow without rebuilding the intake and documentation process pay for it in denials and recoupments.
The consent documentation failure is the one that surprises providers most during audits. They obtained verbal consent. The patient agreed. The visit happened. But CMS does not accept verbal consent as sufficient, and neither do most commercial payers. Written documentation of consent, captured before or at the time of service, is a hard requirement. I have seen practices with otherwise clean billing practices face significant recoupment demands because this one element was missing from hundreds of records.
The payer crosswalk is the tool I recommend most consistently, and the one most practices skip because it takes time to build. A one-page reference document for each payer, listing the accepted codes, required modifiers, POS rules, and documentation checklist, eliminates the guesswork that causes denials. Update it every quarter. Assign one person to own it. The administrative cost of maintaining that document is a fraction of the cost of a single audit.
Telehealth policy is also still moving. CMS updates its telehealth coverage list annually, and commercial payers adjust their policies independently. Staying current is not a one-time task. It requires a scheduled review process, not just a response to denials after they arrive.
— Guorui
Telehealth billing support through Helloklarity
Helloklarity connects patients with over 1,000 licensed providers across mental health, weight loss, and primary care, all through a telehealth platform built for same-day access. For billing specialists managing telehealth service claims, understanding the range of services delivered through platforms like Helloklarity helps contextualize the CPT codes and documentation requirements covered in this guide. Helloklarity accepts major insurance plans and health savings accounts, which means the payer-specific billing rules discussed here apply directly to claims submitted for Helloklarity-facilitated care. Explore the full range of conditions treated through Helloklarity’s provider network to understand the billing contexts your team may encounter.
FAQ
What CPT codes are most commonly used for telemedicine billing?
CPT codes 99202 through 99215 are the most frequently used telehealth billing codes, covering office or outpatient E/M visits for new and established patients. Behavioral health visits use codes 90832 through 90837, and telephone-only visits use 99441 through 99443.
What is the difference between POS 10 and POS 02 for telehealth?
POS 10 designates the patient’s home as the service location and was introduced in 2022 for home-based telehealth. POS 02 applies when the patient is at a non-home originating site such as a clinic or health center. Using POS 02 for home visits results in lower facility-rate reimbursement.
When should modifier 95 vs. modifier 93 be used?
Modifier 95 applies to synchronous audio-video telehealth visits and is preferred by CMS for Medicare Advantage and most commercial payers. Modifier 93 applies to audio-only visits. Some Medicaid programs still require the legacy GT modifier, so payer verification is required before billing.
What documentation is required to avoid telehealth claim denials?
Claims require documented patient location, technology platform, provider location, medical necessity for the telehealth modality, and written informed patient consent captured before or at the time of service. Missing any of these elements is the leading cause of denial and audit recoupment.
Do commercial payers follow the same telehealth billing rules as Medicare?
No. Commercial payers vary widely in their telehealth coding requirements, accepted modifiers, and documentation standards. Applying Medicare rules to commercial claims is a primary cause of denials, making payer-specific crosswalk frameworks a necessity for billing accuracy.
Recommended
- Does Insurance Cover Telehealth? What Every Major Plan Actually Covers In 2026 | Klarity Health, Inc
- Does Blue Cross Blue Shield Cover Telehealth? What Patients Need To Know In 2026 | Klarity Health, Inc
- What Telehealth Services Can I Get Online? Medical Guide
- How Telehealth Prescriptions Work In 2026
Get expert care from top-rated providers
Find the right provider for your needs — select your state to find expert care near you.
Related posts





— Monday to Friday, 7:00 AM to 4:00 PM PST
Join our mailing list for exclusive healthcare updates and tips.

— Monday to Friday, 7:00 AM to 4:00 PM PST